The biggest clinical mistake in professional whitening isn't using the wrong technique — it's reaching for the wrong gel concentration for the case. Stronger isn't always better. Here's how to match HP gel strength to client case type, provider experience level, and treatment goals.
How to Think About Gel Concentration Selection
Professional whitening gel concentration selection should follow one principle: use the lowest concentration that is clinically appropriate for the case — not the highest available. Stronger gel doesn't automatically produce better results. It produces higher sensitivity, greater soft tissue risk, and more demanding protocol requirements. Match the gel to the case.
1. What type of staining does this client have? (Extrinsic vs intrinsic — this determines ceiling expectations)
2. Does this client have a sensitivity history? (Prior whitening sensitivity, dental sensitivity, recession)
3. What is my experience level with isolation protocol? (Directly affects which concentrations are safe to administer)
4. What is the service setting? (In-office clinical vs spa/salon vs studio — affects appropriate concentration range)
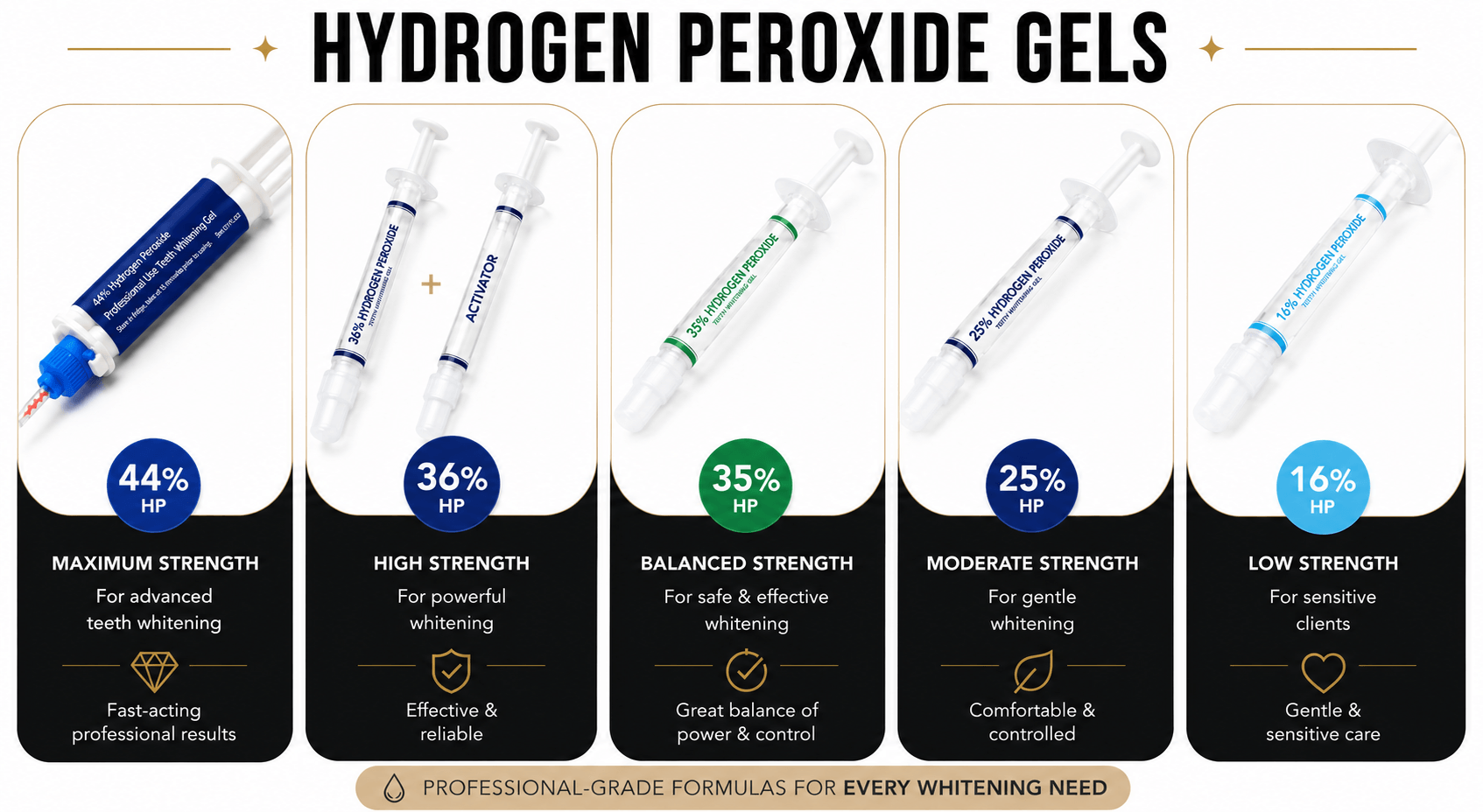
When to Use Each HP Concentration
- Best for
- First-time whitening clients, sensitivity-prone individuals, maintenance sessions after previous whitening
- Stain type
- Mild to moderate extrinsic staining
- Gingival barrier
- Recommended
- Provider experience
- All levels — appropriate for providers building their whitening practice
- Sensitivity profile
- Low — most tolerable HP concentration
- Syringe yield
- 2–3 clients per 1.2 mL syringe
- Best for
- Routine chairside whitening for most clients. The default professional starting strength.
- Stain type
- Moderate extrinsic staining — coffee, tea, tobacco, food
- Gingival barrier
- Strongly recommended
- Provider experience
- All professional levels. Standard concentration for med spas, salons, whitening studios.
- Sensitivity profile
- Moderate
- Syringe yield
- 2–3 clients per 1.2 mL syringe
- Best for
- Heavy extrinsic staining, step-up from 25% HP when results weren't sufficient, experienced providers
- Stain type
- Moderate to heavy extrinsic staining
- Gingival barrier
- Required
- Provider experience
- Experienced with isolation protocol. Not recommended as a starting concentration for new providers.
- Sensitivity profile
- Moderate to high
- Syringe yield
- 2–3 clients per 1.2 mL syringe
- Best for
- Advanced cases where fresh-mix delivery is preferred over single-syringe at similar concentration
- Stain type
- Heavy extrinsic and some intrinsic staining
- Gingival barrier
- Required
- Provider experience
- Advanced — familiar with dual-barrel tip protocol and waste accounting
- Sensitivity profile
- Moderate to high
- Syringe yield
- 2–3 clients (dual-barrel format)
- Best for
- Complex cases: intrinsic staining, tetracycline discoloration, fluorosis, cases where 35% HP has been insufficient
- Stain type
- Stubborn intrinsic and deep extrinsic staining
- Gingival barrier
- Required — strict soft tissue isolation
- Provider experience
- Experienced professionals. Clinical settings preferred. Not a default concentration for routine use.
- Sensitivity profile
- High
- Syringe yield
- Up to 3 clients per 5 mL dual-barrel syringe
Concentration Selection Quick Reference
| Clinical Scenario | Recommended Concentration | Why |
|---|---|---|
| First whitening appointment, unknown sensitivity | 16% or 25% HP | Conservative starting point; assess response before escalating |
| Routine whitening, most adult clients | 25% HP | Balanced between results and sensitivity management |
| Heavy coffee/tea/tobacco staining | 25–35% HP | Stronger concentration for surface-level stubborn staining |
| Previous 25% session didn't reach shade goal | 35% HP | Step up to next concentration with proper isolation |
| Tetracycline or fluorosis discoloration | 44% HP | Maximum-strength for intrinsic staining that surface whitening can't fully address |
| Maintenance after prior whitening series | 16% HP | Lower concentration for maintenance — reduce cumulative sensitivity and cost |
| Sensitivity-prone client, wants whitening | 16% HP with desensitizing prep | Lowest concentration with pre-treatment desensitizing protocol |
| Advanced case, want fresh-mix precision delivery | 36% or 44% HP dual-barrel | Dual-barrel format for maximum potency at placement |
Whitening Gel Strength FAQ
What concentration of hydrogen peroxide is used in professional whitening?
Professional teeth whitening uses hydrogen peroxide at concentrations ranging from 16% to 44%, depending on the case, provider training, and treatment goal. The most commonly used professional concentration for routine chairside whitening is 25% HP. For complex or stubborn cases, 35%, 36% dual-barrel, or 44% dual-barrel HP are used with appropriate isolation protocol. Consumer OTC whitening products typically contain 3%–10% HP or carbamide peroxide equivalents — significantly lower than professional concentrations.
Is stronger whitening gel always better?
No. Stronger gel increases sensitivity risk, soft tissue risk, and protocol demands without necessarily improving results for all cases. Routine extrinsic staining responds well to 25% HP. Using 44% HP for the same case adds sensitivity and risk without adding clinical benefit. Stronger gel is better for cases where weaker concentrations have been insufficient — not as a default for every client.
What is the difference between 25% and 35% hydrogen peroxide whitening gel?
Both are professional chairside concentrations. 25% HP is the most widely used standard professional strength, appropriate for most clients and provider experience levels. 35% HP is the step up for clients where 25% HP hasn't produced adequate results or for heavy extrinsic staining cases. At 35% HP, gingival barrier is required rather than just strongly recommended, and sensitivity management demands increase.
When should I step up from one concentration to the next?
Step up when: (1) the previous concentration didn't achieve the shade goal after a complete properly administered session; (2) the client's stain type is unlikely to respond to the current concentration (intrinsic staining typically needs higher HP); (3) the provider is experienced enough to administer the higher concentration with correct protocol. Don't step up based on impatience or client pressure — step up based on clinical case criteria.
What concentration should a new whitening provider start with?
New professional whitening providers should start with 16% or 25% HP. These concentrations provide professional results while being more manageable in terms of isolation demands and sensitivity risk as you build experience with isolation protocol, session timing, and client management. Starting at 35% or 44% HP without adequate experience is both a client safety risk and a protocol risk.
See the Professional Whitening Safety & Compliance Guide for complete provider training considerations.